
Ventilation & Intubation
Choose from a wide range of high-quality products on the subject of Ventilation and intubation from renowned manufacturers such as Dräger, HUMMcGrath or Rüsch / Teleflex.






143 Products
filter

AERObag® PVC respiratory mask disposable size 0-5 ISO connection

McGRATH MAC Disposable spatula for video laryngoscope optical polymer sterile, various sizes sizes
McGRATH battery 3.6 V disposable battery for video laryngoscope (all models)


VBM Laryngeal Tube LTS-D Disposable Laryngeal Tube latex-free with syringe 1 piece

Ambu Spur II disposable resuscitation bag with O2 reservoir 2600 ml and disposable face mask


Rüsch® Super Safety Clear endotracheal tube


Ambu Disposable Resuscitator Mask Plus latex-free with cuff valve size 1-6


AEROpart oxygen nasal cannula PVC, kink-proof O2 hoses, various nosepieces
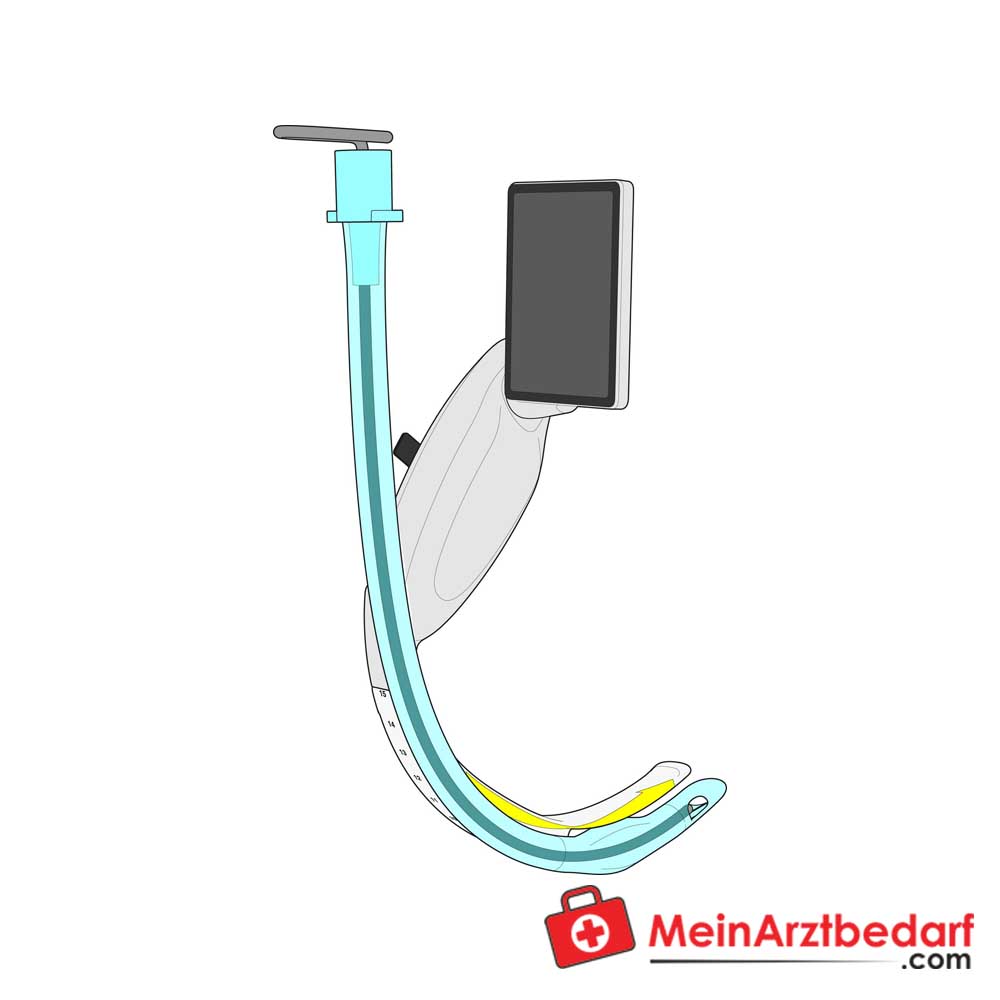

McGRATH Spatula X Blade X3 for video laryngoscope - Intubation spatula


Ambu AuraOnce disposable laryngeal mask latex-free sterile with cuff pressure indicator


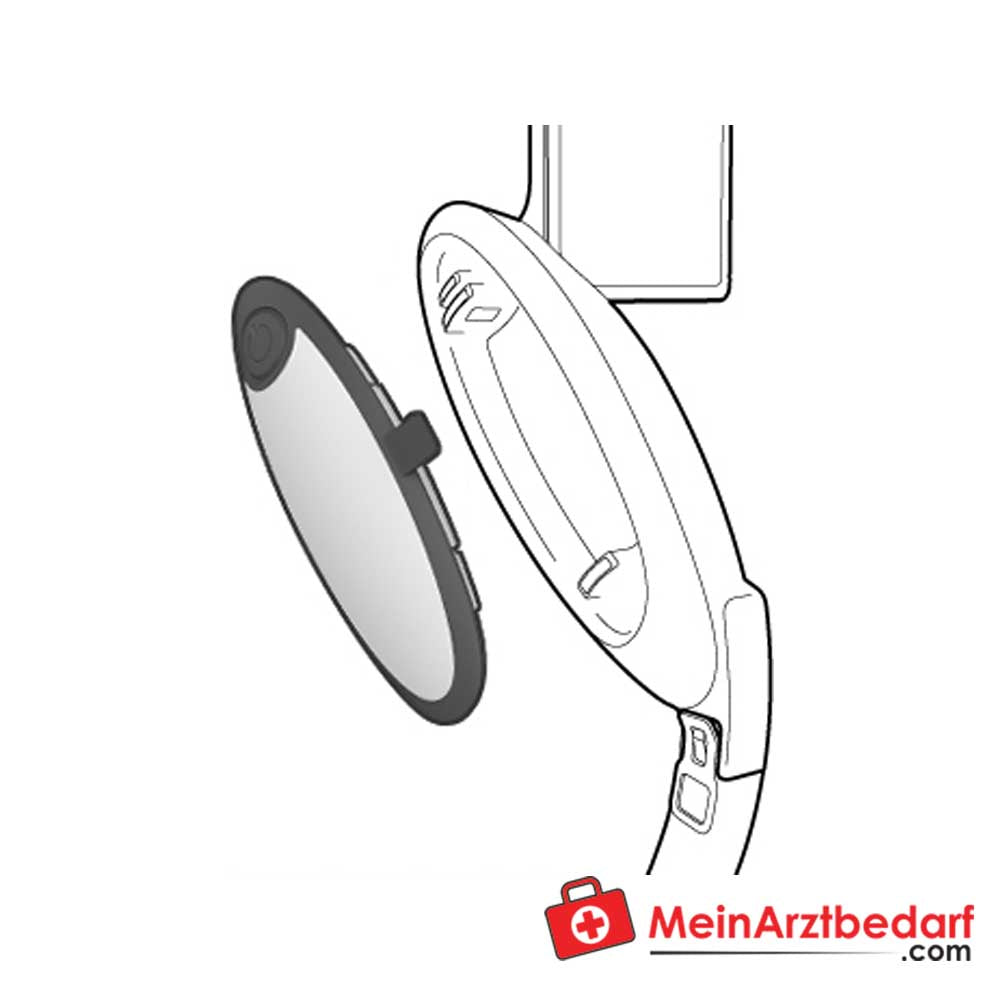
McGRATH transport case for MAC video laryngoscope robust protective case with double zip and fabric carrying handle

RÜSCH Guedel oropharyngeal tube made of PVC

RÜSCH Wendl nasopharyngeal tube made of Wirupren


Dräger Drainage basket Disposable absorber CLIC system, 6 pcs.

AERObag® hyperventilation mask Single use 2000 ml rebreathing bag


AERObag® PVC/PE reservoir bag, 25 mm polycarbonate connection, 2500 ml (adults/children) & 600 ml (baby)


Dräger silicone anaesthesia mask reusable transparent ergonomic handle sizes 00-5


Dräger ClassicStar NIV full face mask, size S-L, 5-point headgear, disposable

Rüsch® Flexislip Super Safetyclear tracheal tube PVC, low-pressure cuff, latex-free, sterile


AERObag® PVC resuscitation bag disposable transparent non-slip swivelling connection adult/child/baby


AEROtreat® safety trolley 10 l oxygen cylinder, 91 cm, 5 castors Ø50 mm
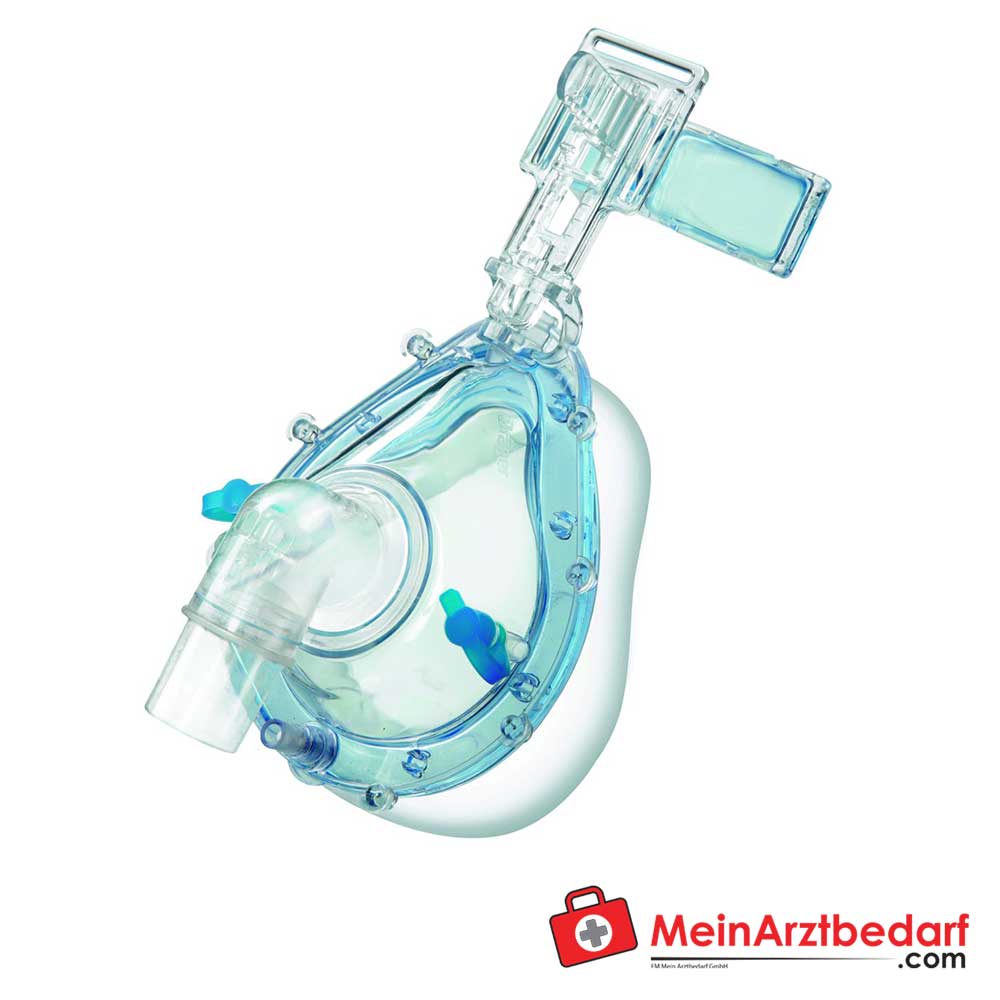
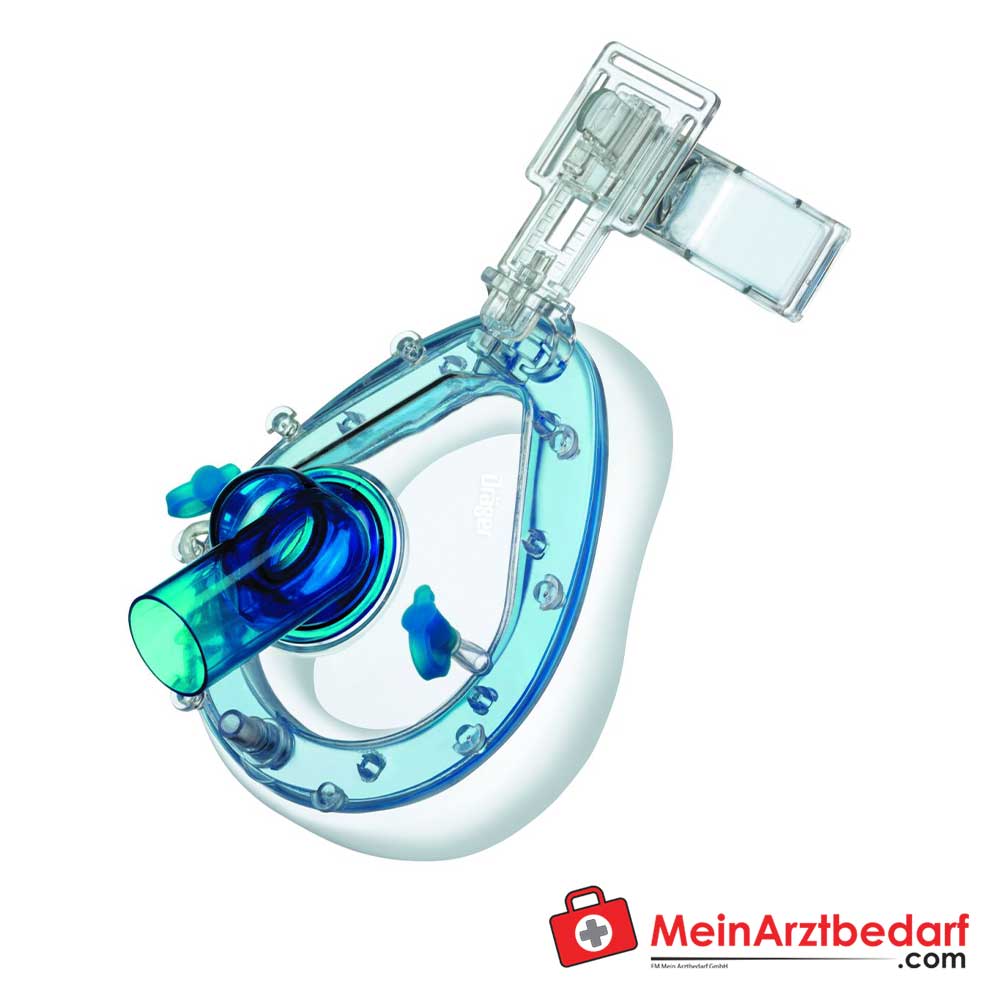
Dräger ClassicStar NIV mask disposable, 6-point headgear, adjustable mask cushion, 360° elbow, sizes S/M/L

Shiley tracheostomy tube for newborns and infants with TaperGuard cuff, transparent retaining plate


AEROtube® disposable endotracheal tubes with cuff, Magill tip & Murphy eye, 15 mm ISO, control balloon, PVC, sterile, 10 pieces
liquid section can be used to create quick custom solutions
Mechanical ventilation
Mechanical ventilation or assisted ventilation is the medical term for artificial ventilation, in which mechanical means are used to support or replace spontaneous breathing. This can be a device called ventilation device, or breathing can be supported manually by a correspondingly qualified specialist, such as an anesthetist, respiratory therapist or paramedic, by pressing a bag valve mask.
Mechanical ventilation is called "invasive" when it affects an instrument within the trachea through the mouth, such as an endotrache alubus or skin, such as a tracheostomy tube. Facial or nose masks are used for non-invasive ventilation in the case of non-selected non-unconscious patients.
The two most important types of mechanical ventilation are the overpressure ventilation, in air (or another gas mixture) through the airways into the lungs, and the vacuum ventilation, in which air is essentially sucked into the lungs by stimulating movement of the breast. Apart from these two main types, there are many specific types of mechanical ventilation, and their nomenclature has been revised over the decades in the course of the continuous further development of the technology.
When does a patient have to be ventilated?
Mechanical ventilation is indicated if the patient's spontaneous breathing is not sufficient to maintain life. It is also used as prophylaxis if the collapse of other physiological functions or ineffective gas exchange in the lungs is also used. Since mechanical ventilation only serves to support breathing and does not heal an illness, the basic state of the patient should be identified and treated in order to solve it over time. In addition, further factors must be taken into account, since mechanical ventilation is not uncomplicated.
In general, mechanical ventilation is used to correct blood gases and reduce breathing work.
The usual medical indications for the application include:
- Acute lung damage, including acute respiratory nympia (ARDS) and trauma.
- Apnea with respiratory arrest, including cases of intoxication
- Acute heavy asthma that requires intubation.
- Acute in chronic airway acidosis, most often in chronic obstructive lung disease (COPD) and obesity hypoventilation syndrome.
- Acute respiratory acidosis with carbon dioxide partial printing (PCO2)> 50 mmHg and ph <7.25, which can be attributed to paralysis of the diaphragm by the Guillain-Barré syndrome, myastenia gravis, motor neuron diseases, spinal cord injuries or the effect of naxwork and muscle relaxation.
- Increased breathing work, as shown by significant tachypnea, retraction and other physical signs of shortness of breath.
- Hypoxemia with arterial oxygen partial pressure (PAO2) <55 mm Hg with an additional proportion of inspired oxygen (FIO2) = 1.0
- Hypotony including sepsis, shock, congestive heart failure
- Neurological diseases such as muscular dystrophy and amyotrophic lateral sclerosis (ALS)
Risks:
- Barotrauma - Lung baro trauma is a well -known complication of mechanical overpressure ventilation. This includes pneumothorax, subcutaneous emphysema, pneumomediatinum and pneumoperitoneum.
- Ventilation -associated lung damage - Beating -associated lung damage (vali) relate to acute lung damage that occurs in mechanical ventilation. It cannot be distinguished clinically from acute lung injury or acute respiratory nympia (Ali/ARDS).
Complications:
Mechanical ventilation is often a life -saving intervention, but has potential complications such as pneumothorax, respiratory injuries, alveolar damage and breathing associated pneumonia. Further complications are membranetrophy, reduced cardiac volume and oxygen toxicity. One of the primary complications occurring in mechanically ventilated patients is the acute lung injury (ali)/acute respiratory nympia (ARDS). Ali/ARDS are recognized as significant contributions to the morbidity and mortality of the patients.
In many health systems, long -term ventilation as part of intensive care medicine is a limited resource (since there are only so many patients who can be cared for at any time). It is used to support a single failing organ system (the lungs) and cannot reverse a underlying disease process (e.g. cancer in the final stage). For this reason, there can be (occasionally difficult) decisions about whether it is suitable to start with mechanical ventilation. Just as many ethical questions concern the decision to cease mechanical ventilation.
The design of the modern overpressure fans were mainly based on technical developments in the military during the Second World War to supply the oxygen of fighter aircraft at great height. Such ventilation devices replaced the iron lungs because safe endotrachealt tubes with cuffs with high volume/low pressure were developed. The popularity of overpressure fans rose in Scandinavia and the USA during the polio epidemic in the 1950s and was the beginning of modern ventilation therapy. The overpressure by manual supply of 50% oxygen via a tracheostomy cannula led to a reduced mortality rate in patients with polio and respiratory paralysis. Due to the enormous personnel requirement for such manual interventions, mechanical overpressure fans have become increasingly popular.
Overpressure ventilation devices work by increasing the patient's respiratory pressure through an endotracheal or tracheostomic hose. The overpressure lets air flow into the airway until the ventilation of the ventilation device is over. Then the respiratory pressure drops to zero, and the elastic recoil of the breast wall and lungs press the tidal volume - exhalation through passive exhalation.
The time of withdrawal from mechanical ventilation - also called weaning or weaning - should be carefully weighed. Patients should consider their ventilation for the withdrawal if they are able to support their own ventilation and oxygen supply, and this should be assessed continuously. There are several objective parameters that you have to look for if you think about a withdrawal, but there are no specific criteria that generalize themselves to all patients.
One of the main reasons for the admission of a patient to an intensive care unit is the implementation of mechanical ventilation. The monitoring of a patient in mechanical ventilation has many clinical applications: improvement in understanding pathophysiology, help in diagnosis, guidance for patient management, avoidance of complications and evaluation of trends.